

Head Gear That Will Provide 2010 Visual Acuity UPDATED
Head Gear That Will Provide 2010 Visual Acuity
You've finally arrived.
Undergrad, MCAT, medical school, Footstep 1. Ruby-red eye flights as y'all interviewed for residency. The stress of early Jan match when all your friends were relaxing on radi-holiday. And so the elation of match! Your early retirement from med school!
And at present yous are here, walking into clinic on your first twenty-four hour period of ophthalmology residency. Yous choice up the chart exterior the door: Cataract evaluation. Simple every bit that…find it, fix it, right?
Non so fast. What type? What grade? What tests? Does the patient see indications?
This framework will provide the high level overview.
Cataract Type
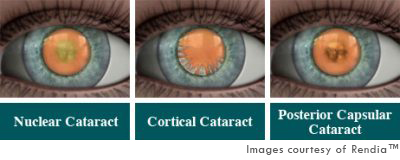
There are three primary types of cataracts that represent 99% of the cataracts that you will encounter in clinic. Sure, kids will take congenital cataracts, and certain medications or systemic conditions will effect in special cataracts, merely these are not important to know at this point.
Cataracts types are defined by where the opacities be within the lens and graded by how severe the opacities are at that location.
- Nuclear sclerotic cataract (NS) – Cloudiness of the nucleus, the central portion of the lens.
- Cortical spoking cataract (CS) – Swelling of the cortex causing spoke/wedge-like peripheral cloudiness.
- Posterior subcapsular cataract (PSC) – Opacity in the posterior capsule of the lens, oftentimes seen in younger individuals, steroid users, and diabetics. All else beingness equal, these are commonly the most visually significant.
Cataract Grading
At present that you know the types, how do you communicate their severity to others? This is a poorly defined topic. Some clinicians become with their gut feel. Others use visual vigil every bit a rough guide.
Cataract grading is important because patients will often requite a very nebulous complaint well-nigh their vision getting worse, and it volition be your job to effigy out why. A cataract is often the cause, and just an authentic prior grading can help you lot decide whether the cataract has actually changed since the last visit. If it hasn't, and so you need to await for other causes of vision loss. Having a reliable grading organization helps immensely.
In addition, surgical complication rates in training programs are high (up to 5% of cases vs. 0.2% post-training), and it is important to weigh the run a risk of surgery versus the potential benefit. For case, if a patient has both a cataract and macular degeneration, they may non actually do good from surgery if the cataract is mild (Grades 1-2+). Knowing how much yous would expect a cataract to affect vision helps you lot determine whether cataract surgery is worth the risk.
Finally, almost programs aim to have third year residents hang out primarily in the operating room. They often won't personally evaluate every patient before surgery. As a junior resident, you need to be able to accurately convey the characteristics of a cataract to your seniors so that they can determine the approach, plan which cases should go to less or more experienced residents, and anticipate surgical complications.
In 2002, The WHO published a simplified cataract grading scale. These images are directly from that paper:
Nuclear sclerotic (NS)
Best graded with slit axle at thirty to 45 caste angle to the cataract. In an early cataract, y'all volition see that the primal nucleus is actually more clear than the inductive and posterior embryonic layers of the lens:
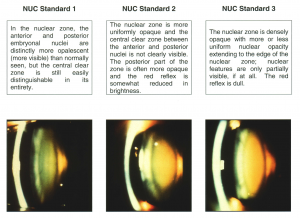
NS tr or 1+: Nucleus clearer than anterior/posterior sections
NS ii+: Nucleus equal to the anterior/posterior sections (same opacity level throughout)
NS 3+ Nucleus denser than anterior/posterior sections
NS iv+ Brunescent: Cataract completely opaque/chocolate-brown
Cortical spoking (CS)
Best graded while visualizing with retroillumination. It may be difficult to retroilluminate if at that place is a concurrent NS cataract. By WHO criteria, think of the lens equally a pizza and sum up the area of the peripheral spoke like opacities.

CS 1+: ⅛ to ¼ of the total area
CS 2+: ¼ to ½ of the total expanse
CS 3+: ½ or more of the total area
Posterior subcapsular cataract (PSC)
Also best graded while visualizing with retroillumination. Like CS, PSC may be hard to retroilluminate if there is a dumbo concurrent NS cataract.WHO criteria, graded on vertical height (in mm)

PSC 1+: one mm to 2 mm
PSC 2+: 2 mm to 3 mm
PSC 3+: >three mm
These basic measurements are combined into a cataract grade. You tin have multiple types of cataracts at once and this tin can be written every bit the following:
OD: two+ NS, two+ CS, ane+ PSC
Os: 2+ NS, one+ CS
Visual acuity
Across the cataract course, in that location is a minimum visual acuity that is by and large indicated for surgery. This varies from one preparation program to the next, and it is used to weigh the benefit of surgery vs. the high complication rate of residents. Some attendings in practice will do cataract surgery on 20/xxx, 20/25, and even twenty/20 optics if glare or night symptoms exist! This is Not our goal in grooming as our complication rates may exist up to 50x college than those of a veteran surgeon.
In most residency training programs, we aim for vision worse than 20/forty to xx/fifty every bit a prerequisite for cataract surgery, forth with symptomatically decreased vision. This vision can consequence from a combination of the above cataract types. It's also important to dominion out retinal and corneal etiologies of decreased vision earlier starting preop testing to maximize your chances of improving visual acuity postoperatively.
Once we determine that a patient needs surgery, we are fix for pre-op testing.
Treatment
Treatment of cataracts is surgical. Although at that place are rumblings every few years about eyedrops which dissolve cataracts, there are not yet any evidence-based treatments except surgery. The almost commonly performed cataract performance is phacoemulsification. Newer methods augment phacoemulsification with femtosecond laser, but these practice non drastically modify the underlying procedure.
Practice grading cataracts below, and so click hither to learn how to do pre-op testing and mail-op evaluations.
Conclusions
- These 3 types of cataracts embrace 99% of the cataracts that y'all will see in clinic: nuclear sclerosis (NS), cortical spoking (CS), and posterior subcapsular (PSC).
- Each cataract subtype is graded depending upon its severity by WHO criteria.
- Indications for surgery include: 20/40 vision or worse (varies by institution) and symptoms such as glare/halo/photosensitivity.
- Complication rates in grooming programs are higher than boilerplate. Knowing how to grade cataracts will ensure that the surgery you lot are planning is worth the gamble.
References
- Thylefors B, Chylack LT, Konyama K et al. A simplified cataract grading system. Ophthalmic Epidemiology 2002
Your Score:
Your Ranking:
DOWNLOAD HERE
Head Gear That Will Provide 2010 Visual Acuity UPDATED
Posted by: kristinkinty1970.blogspot.com

Comments
Post a Comment